

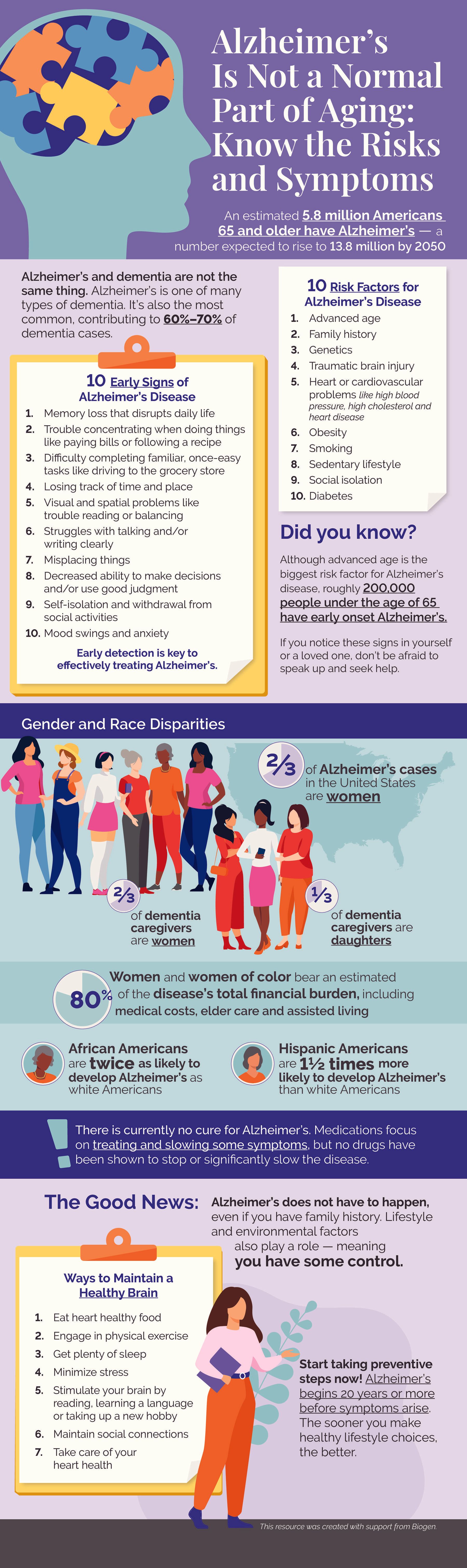
An estimated 5.8 million Americans age 65 and older have Alzheimer’s — a number expected to rise to 13.8 million by 2050.
Did you know?
Alzheimer’s and dementia aren’t the same thing. Alzheimer’s is one of many types of dementia. It’s also the most common, contributing to 60%-70% of dementia cases.
10 risk factors for Alzheimer’s disease
- Advanced age
- Family history
- Genetics
- Traumatic brain injury
- Heart or cardiovascular problems like high blood pressure, high cholesterol and heart disease
- Smoking
- Sedentary lifestyle
- Social isolation
Did you know?
Although advanced age is the biggest risk factor for Alzheimer’s disease, roughly 200,000 people under the age of 65 have early onset Alzheimer’s.
10 early signs of Alzheimer’s disease
- Memory loss that disrupts daily life
- Trouble concentrating when doing things like paying bills or following a recipe
- Difficulty completing familiar, once-easy tasks like driving to the grocery store
- Losing track of time and place
- Visual and spatial problems like trouble reading or balancing
- Struggles with talking and/or writing clearly
- Misplacing things
- Decreased ability to make decisions and/or use good judgment
- Self-isolation and withdrawal from social activities
- Mood swings and anxiety
If you notice these signs in yourself or a loved one, don’t be afraid to speak up and seek help. Early detection is key to effectively treating Alzheimer’s.
Gender and race disparities
- Women make up ⅔ of Alzheimer’s cases in the United States
- African Americans are twice as likely to develop Alzheimer’s as white Americans
- Hispanic Americans are 1½ times more likely to develop Alzheimer’s than white Americans
- Women and women of color bear an estimated 80% of the disease’s total financial burden, including medical costs, elder care and assisted living
⅔ of dementia caregivers are women | ⅓ of dementia caregivers are daughters |
There is currently no cure for Alzheimer’s. Medications focus on treating and slowing some symptoms, but no drugs have proven effective in stopping or significantly slowing the disease.
The Good News: Alzheimer’s doesn’t have to happen, even if you have a family history. Lifestyle and environmental factors also play a role — meaning you have some control.
Ways to maintain a healthy brain
- Eat heart healthy food
- Engage in physical exerciseGet plenty of sleep
- Minimize stress
- Stimulate your brain by reading, learning a language or taking up a new hobby
- Maintain social connections to lower the risk of cognitive decline
- Take care of your heart health
Start taking preventive steps now! Alzheimer’s begins 20 years or more before symptoms arise. The sooner you make healthy lifestyle choices, the better.
Did you know?
More than a third of global dementia cases can be avoided through a healthy lifestyle, according to a 2017 study.
This resource was created with support from Biogen.





